If you are taking anti-coagulation (blood thinning) medication e.g. warfarin then you will need to stop this for approximately 5 days prior to your procedure. Your doctor may arrange for you to have daily heparin injections after you stop the warfarin.
Patients will be required to attend the pre-admission clinic on the day prior to the procedure.
At the pre-admission clinic you will see a doctor who will record your medical history. You will also require an ECG and blood test. The doctor will also confirm the time you should be at the hospital for admission the following day.
You will be required to fast for at least six hours before each of the procedures. If your procedure is in the afternoon you may have a light breakfast. If your procedure is in the morning, DO NOT EAT OR DRINK AFTER MIDNIGHT, except for sips of water to help you swallow your pills.
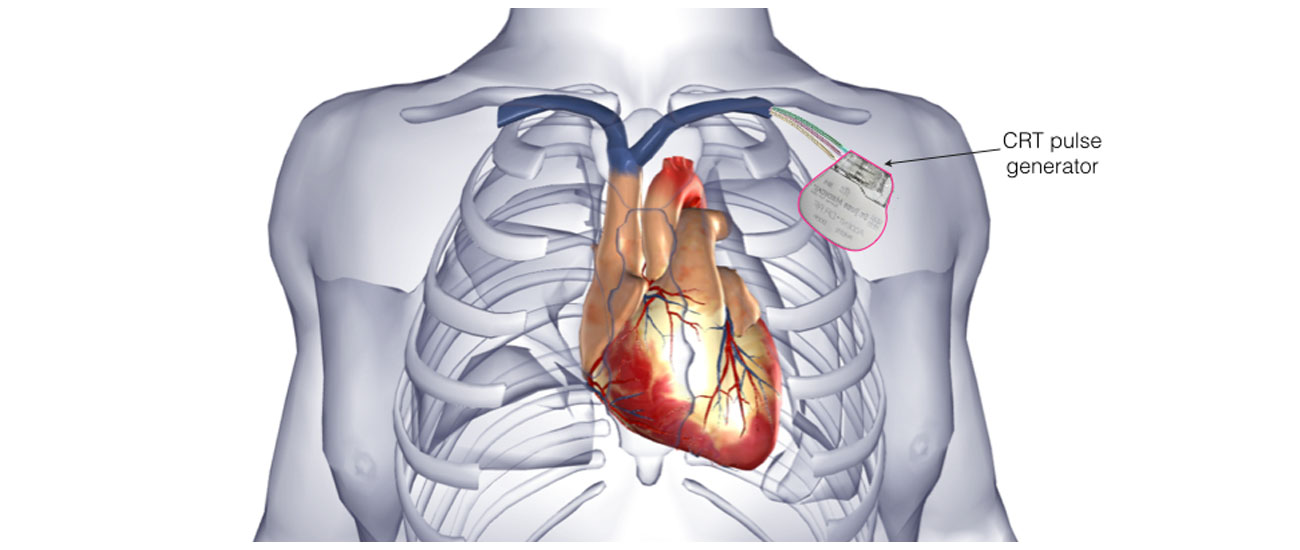
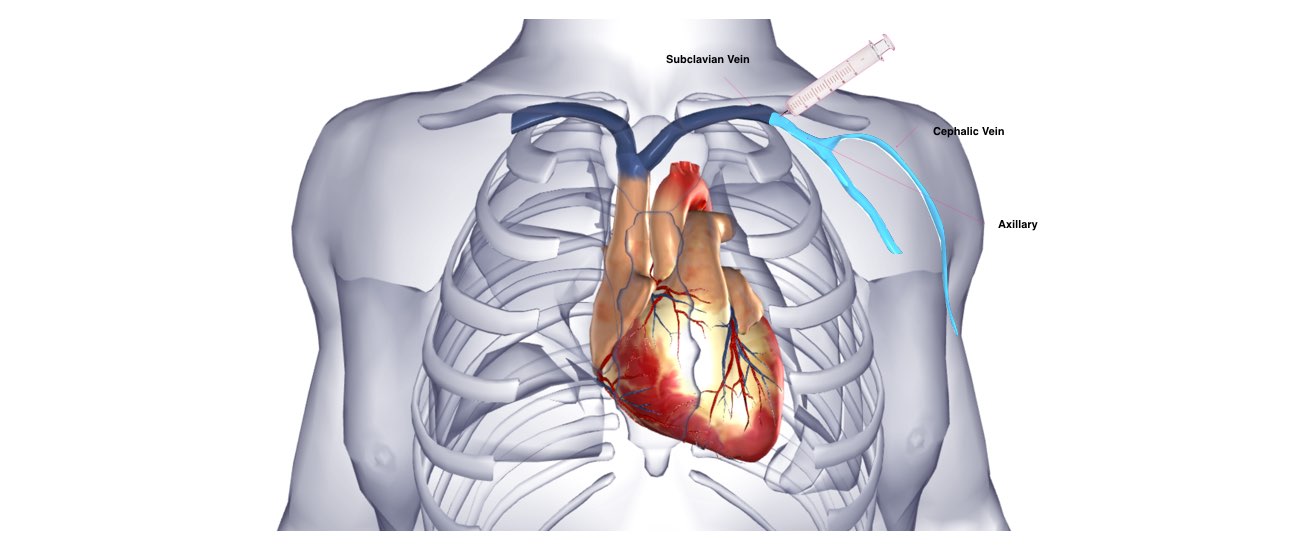
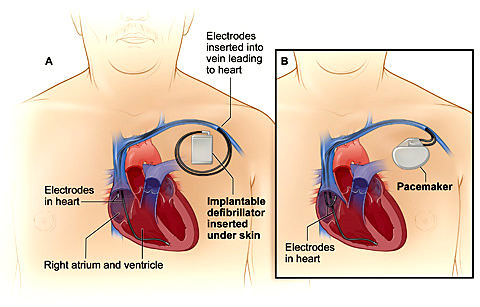
Insertion of a CRT device is now a very common procedure. This is performed either under local anaesthetic with sedative medication to make you feel comfortable or under general anaesthetic. Your doctor will discuss this with you. The procedure takes approximately 2 hours and is performed in the cardiac catheter laboratory.
This is a special room that has a patient table, X-Ray tube, ECG monitors and other equipment. The staff in the lab will all be dressed in hospital theatre clothes and during the procedure will be wearing hats and masks.
Many ECG monitoring electrodes will be attached to your chest area. A nurse or doctor will insert an intravenous line usually into the back of your hand. This is needed as a reliable way to give you medications during the study without further injections. You will also have a blood-pressure cuff attached to your arm that will automatically inflate at various times throughout the procedure.
After the procedure you will have some bruising and discomfort in the area of the CRT device that may persist for several weeks. This bruising can create a bluish discoloration over the upper chest and arm. This is normal.
You should avoid strenuous activities with your arm or from lifting the arm above your head for a period of 4 weeks. You should refrain from driving for 2 weeks. If you have already had a heart rhythm disturbance you may be disqualified from driving for 6 months. Your doctor will discuss this with you. You should not go swimming, play golf, or bowling for 4 weeks.
A sterile dressing is left over the pacemaker for 8 days. You can carefully remove this dressing yourself on the 8th day after the procedure. At this stage the wound is sufficiently healed to allow you to shower with the dressing removed.
You will be allowed to go home 1 or 2 days after the procedure.
You will be given an appointment to see the doctor 1 month after the implant.
Usually the discomfort and swelling from the wound settles gradually over several weeks. If the wound becomes increasingly tender, reddened and swollen or you have any other concerns, you should contact your cardiologist.